Department of Cardiovascular Biology and Medicine,
Juntendo University Graduate School of Medicine
Associate ProfessorMiho Yokoyama
The benefits of cardiac rehabilitation on the prevention of recurrence and improvement of QOL after suffering from cardiovascular diseases have become clear. Juntendo University has been focusing on and practicing cardiac rehabilitation for 20 years. In collaboration with experts from the Faculty of Health and Sports Science, the Faculty of health care and Nursing, and the Faculty of Health Science, we will develop a multifaceted and comprehensive program tailored to each individual patient from a scientific perspective and provide long-term support. We aim to offer personalized medical care that will support for a lifetime.
Aiming to become a doctor of cardiovascular medicine to support the life of patients suffering from chronic diseases
The heart is the only beating organ in the body and I found it intriguing to be able to see it with my own eyes. What makes this field worthwhile is that medical operations are also performed, providing opportunities for doctors to interact postoperatively with the patients on an ongoing basis. At first, I became interested in acute phase treatment such as catheter intervention. However, with progress in acute phase cardiovascular treatment, chronic phase treatment and prevention of recurrence have also become major topics. In cardiovascular care, treatment technology for the acute phase has evolved and the mortality rate has declined. However, as the number of elderly people with chronic diseases such as heart failure is increasing, I strongly felt the need to implement follow-up care.
During my school days, I enjoyed good health. Therefore, even after becoming a trainee, I could not empathize with the patients, which disturbed me greatly. However, after starting to work as a doctor, I began to suffer from dizziness due to Meniere's disease and was placed in a painful situation of having to deal with a chronic disease. Meanwhile, a doctor gave me several advises on how to work and how to live, which provided me with a great comfort at that time. This piqued my interest and motivation for studying chronic diseases.
Developing a keen interest in cardiac rehabilitation where patients can be treated according to their own efforts
Cardiac rehabilitation began to be implemented at Juntendo University more than 20 years ago. In 2006, chronic heart failure, macrovascular disease, and peripheral arterial occlusive disease were newly included in the scope of cardiac rehabilitation insurance. After experiencing my own illness, I was assigned to a ward as a cardiologist where I extensively worked with patients suffering from various illnesses. I was fascinated by the treatment of cardiac rehabilitation in which the patients' own efforts are supported for many years. Furthermore, I was provided with the opportunity to become involved in the launching of cardiac rehabilitation at Juntendo University Urayasu Hospital when I was a cardiovascular specialist. It was then that I decided to devote myself to cardiovascular medicine as a subspecialty.
While there is much evidence in support of cardiac rehabilitation, my goal was to specifically verify why it is effective in preventing the recurrence of ischemic heart disease. Intervention which dilates and cures blood vessels with a catheter has great impacts. Likewise, with cardiac rehabilitation, if an image displaying changes in arteriosclerosis can be shown, the patients can sense the effect by seeing it with their own eyes. Therefore, my goal is to introduce our research on how cardiac rehabilitation, especially exercise therapy, is effective for arteriosclerosis.
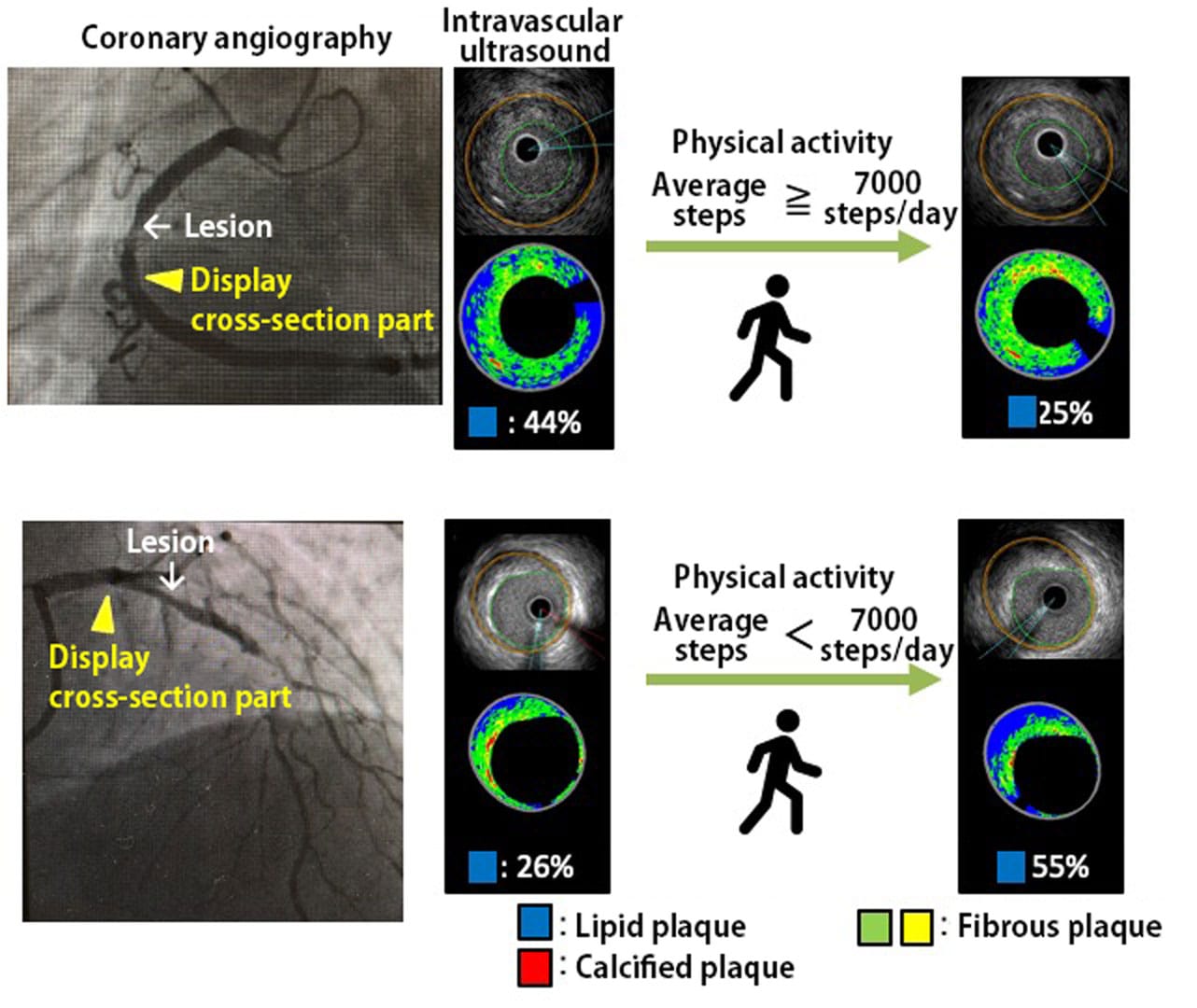
After giving intervention treatment to patients suffering with acute coronary syndrome, cardiac rehabilitation was performed during hospitalization, and an exercise prescription was created from the results of cardiopulmonary exercise test. At the time of discharge, discharge guidance including the recommended amount of daily activity was given and the patients were encouraged to participate in outpatient cardiac rehabilitation. According to the amount of daily activity of patients after their discharge, the patients were divided into two groups; those with an average of 7,000 steps or more per day and those with an average of less than 7,000 steps per day. Eight months later, we compared the changes in the amount and quality (lipid component) of coronary plaque with intravascular ultrasound. As a result, it was found that the plaque amount had reduced and the lipid component had reduced in the group with 7,000 steps or more as compared with the group with 7,000 steps or less. It came to light that active physical activity not only reduces plaque but also stabilizes it. It is known that myocardial infarction is caused not by the increase of plaque but by the instability and collapse of the plaque. People with myocardial infarction are known to have unstable plaques in body parts other than those treated with intervention. Recurrence cannot be prevented simply by the intervention of blood vessels. Considering that acute myocardial infarction is still increasing, lifestyle improvements including active physical activity and comprehensive cardiac rehabilitation are considered to be one of the major cardiovascular disease therapies. We believe that the results of this study will not only help in spreading clinical exercise therapy, but will also have a significant impact on the health and hygiene of the people from the perspective of preventive medicine. In fact, we used an arteriosclerosis model in our fundamental research, and when we actually made the mice run around the cage, the mice that were moving developed less arteriosclerosis. From this result, we verified that physical activity suppresses arteriosclerosis lesions.
There are still very few cardiac rehabilitation facilities in Japan.
Expectations are rising for the possibility of online collaboration
Cardiac rehabilitation has certain benefits, such as reducing cardiovascular mortality by 26% for ischemic heart disease and reducing re-hospitalization rate by 39% in the case of heart failure. However, it is still not very popular and the implementation rate is likewise low, which poses a problem. The implementation rate of cardiac rehabilitation after angina pectoris, myocardial infarction, and cardiac bypass surgery, which are ischemic heart diseases, is about 30-40% overseas, but very low in Japan at around 4%-8%. In addition, the cardiac rehabilitation implementation rate for heart failure patients in Japan was 7% for both inpatients and outpatients. One problem is that there are very few outpatient facilities for cardiac rehabilitation, and another problem is that only few patients are aware of cardiac rehabilitation. Therefore, I think it is extremely important to increase the number of facilities that perform cardiac rehabilitation, improve its quality and increase its awareness in society. We started cardiac rehabilitation outpatient clinic in 2010, which serves as a contact point for patients in need of cardiac rehabilitation. Even if the patient has undergone heart surgery at another hospital, the patient is able to have cardiac rehabilitation at Juntendo hospital with patient information hared and coordinated. Currently, we also operate a heart failure outpatient clinic in cooperation with the heart failure team. The cooperation between hospitalization and outpatient care has been further strengthened by conducting detailed examination of patients with heart failure after acute phase treatment and patients who have recently been operated on.
A secondary prevention outpatient service that provides health guidance is also available, such as providing health guidance, bodily function examination and exercise routine checkup approximately every 3 months, depending on the medical condition of the patient.
In Japan's highly aging society, patients suffering from myocardial infarction and heart failure are aging. The biggest problem in that situation is frailty. Frailty is a condition in which vulnerability to health disorders increases due to various functional changes and decline of reserve capacity due to aging. This is a condition in which muscle loss (sarcopenia), life dysfunction and abnormalities in immunity and neuroendocrine are involved in a complex manner, resulting in the patient suffering, not only physical but also mental and social frailty. Since frailty worsens the prognosis of patients, the current concept of cardiac rehabilitation incorporates frailty prevention and heart failure disease management which includes exercise therapy, counseling, and patient education to increase exercise tolerance and improve the quality of life for recurrence prevention and long-term prognosis improvement. Until now, overseas data was mostly used due to the lack of data for Japanese people. However, a system has now been put in place so as to make possible gradual accumulation of data for Japanese people. In recent time, we have also been focusing on developing new programs effective for the elderly. Once these results become apparent, the motivation of the patients will proportionately increase, bringing about synergic benefits.
In addition, under a coronavirus infection, many facilities currently reduced the number of sessions providing cardiac rehabilitation. We have created and provided videos of cardiac rehabilitation programs that can be practiced at home. This endeavor allows patients to access and carry out these online programs at home even if they are unable to visit the hospital due to the coronavirus pandemic. Online programs make collaboration with remote facilities possible. The online media provides patients with a sense of security and a feeling of solidary, boosting their motivation. Recently, the monitoring of electrocardiograms etc. has made great progress, providing a wider range of possibilities. 20-40% of heart patients also suffer from depression and anxiety disorders. I was reminded of their need for mental support in addition to physical support. So far, we have held Tai Chi lessons with 50 participants. Going forward, in addition to one-on-one online interaction, I hope to see patients having more interchange among themselves.
The best environment for collaborating with various health experts
As you know, Juntendo University has three faculties, the Faculty of Medicine, the Faculty of Sports and Health Science and the Faculty of Medical Nursing. Cardiovascular Rehabilitation and Fitness Juntendo University was established in 1993 for performing medical checks on patients even if they do not have any illness, and for providing exercise guidance and health guidance with a multidisciplinary team based on an exercise prescription. Currently, at the Health and Sports Section, we have built an excellent environment in which=where medical treatment may be offered and research may be conducted in collaboration with multidisciplinary staffs. In 2019, the Faculty of Health Science was newly established where physical therapists with experience in cardiac rehabilitation are also present. Each of the staff has his / her own specialty and their involvement.
One of the best things about cardiac rehabilitation research is its effect on exercise tolerance. In my clinical practice, I felt that there was a difference in the improvement of exercise tolerance among patients who had undergone coronary artery bypass surgery depending on whether they had diabetes or not; thus, I tried to verify this hypothesis. I found that glycemic control is related to exercise tolerance, muscle strength and muscle mass responses, but this mechanism is one that requires further clarification and scientific investigation. At the Health and Sports Section, we measure advanced glycation end products and also collect and verify various data with the cooperation of patients.
I believe that it is necessary to individually deal with patients to determine which program is most suitable for each patient. The response will vary depending on the frailty of the elderly patient. In the case of pre-frailty patients, a high rate of recovery can be expected with the treatment, thereby making prevention and improvement possible. We have been able to clinically establish that it is more effective to provide the treatment prior to becoming ill.
Factors related to exercise tolerance vary from person to person and various mechanisms are involved in this. We are currently developing a program incorporating new indexes.
Desire to expand the program in collaboration with local sports facilities
Providing scientifically-proven programs and demonstrating indexes understandable for patients will enhance their motivation. I believe that people who have not been able to start or continue exercising until now are becoming more health conscious due to the coronavirus pandemic. If we can provide cardiac rehabilitation programs to local sports facilities and provide opportunities so that exercise therapy may easily be performed anywhere, it will lead to early detection and recurrence prevention. Ultimately, that will lead to the number of people suffering from chronic diseases to decrease.
Our university has also partnered with a local fitness club and has started the initiative of prescribing exercises at the fitness club for persons in the maintenance phase. We have been holding bilaterally regular study sessions for information exchange. I hope to expand programs that can be presented medically to local regions.
Cardiology is a field that provides long-term support to patients from the acute phase to the chronic phase. However, it is cardiac rehabilitation that ultimately improves long-term prognosis and quality of life. I find cardiac rehabilitation fascinating because it starts with prevention and allows me to provide support to the patients for an extended period of time. Cardiac rehabilitation is still under development academically, but it is a fulfilling endeavor as we work to develop the programs. I would be pleased for more people to join us in this field.
Miho Yokoyama
2000 Graduated from Kagawa University School of Medicine.